

A practice of St. Peter’s Health Partners Medical Associates, Albany Cardiothoracic Surgeons is the sole provider of cardiac surgery at St. Peter’s Hospital in Albany, NY. In operation since 1955, it is the oldest heart surgery practice dedicated to cardiothoracic surgery in the Capital Region. With over seven decades of experience providing expert-level cardiothoracic surgery, Albany Cardiothoracic Surgeons has become a core aspect of cardiac care within the larger St. Peter’s health system, as Nicholas Montalto, MD, Chief Medical Officer, Acute Care at St. Peter’s Health Partners explained.
“Cardiothoracic surgery is a critical component of a comprehensive cardiac program at St. Peter’s Health Partners, ensuring that patients have access to a full spectrum of advanced heart care close to home,” Dr. Montalto said. “Beyond individual procedures, cardiothoracic surgery strengthens the overall quality of our regional cardiac program, which covers a wide area beyond the Capital Region – stretching into southwestern Vermont, western Massachusetts, north toward the Canadian border and south to the Kingston area.”
Dr. Montalto highlighted the practice’s four Board-Certified cardiac surgeons who bring extensive expertise in cardiac services, both surgical and procedural: Chief of Cardiothoracic Surgery Chris Rokkas, MD, Sulaiman Hasan, MD, Stephanie Helmer, MD, and Rebecca Phillip, MD. He pointed to the excellent cardiac care offered by the surgeons and their teams as a primary reason St. Peter’s cardiothoracic program has received several accolades over the years, such as being rated as high performing in several heart surgery areas including aortic valve surgery, heart attack and heart bypass surgery. St. Peter’s was also recently named Best Regional Hospital in the Capital Region by U.S. News & World Report, a title it has maintained for twelve consecutive years.
 “The team’s surgical expertise enables them to not only perform traditional CABG (coronary artery bypass graft) procedures, but also virtually any complex cardiac condition,” explained Dr. Montalto. “Our surgeons specialize in repair and replacement of mitral and aortic valves as well as surgery for aortic aneurysms. This expertise is why St. Peter’s cardiac surgery is consistently ranked among the highest quality programs in New York state.”
“The team’s surgical expertise enables them to not only perform traditional CABG (coronary artery bypass graft) procedures, but also virtually any complex cardiac condition,” explained Dr. Montalto. “Our surgeons specialize in repair and replacement of mitral and aortic valves as well as surgery for aortic aneurysms. This expertise is why St. Peter’s cardiac surgery is consistently ranked among the highest quality programs in New York state.”
Wide-Ranging, Complex Heart Surgery to Meet Patients’ Needs
Having held Cardiac Surgery Chief positions at many academic universities, Dr. Rokkas has extensive expertise in complex surgery care, including aortic and mitral valvular replacement and repair, and he specializes in complex aortic surgery. Dr. Rokkas shared why he chose to join St. Peter’s Health Partners in July of 2025.
“I chose St. Peter’s to continue my career because of the great reputation the hospital has and its rich history in cardiac care,” Dr. Rokkas said. “There’s a lot of emphasis on cardiovascular disease, good results, and a good reputation, and that’s why I joined.”
One of the important recent developments with Albany Cardiothoracic Surgeons is the new Aortic Center opening this spring. Dr. Rokkas said this center will directly address the cardiac needs of the community.
“There is a community need for patients with aortic diseases to be followed and treated at a very specialized center. We have the expertise now at St. Peter’s Hospital to treat patients with complex aortic problems. We’re setting up a very specialized and focused clinic that will serve only patients with aortic disease, including aneurysms of the ascending aorta, aortic dissections and other aortopathies,” Dr. Rokkas explained.
Albany Cardiothoracic Surgeons is also focusing on a new heart failure program. A serious disease that kills hundreds of thousands of people each year, heart failure is a major epidemic across the country, Dr. Rokkas said.
 “We are developing a specialized program to treat patients who come in for heart surgery for other conditions like coronary artery disease or heart valve issues and have heart failure,” he said. “We’ll have the technology to care for patients with heart failure at the same time when we’re handling coronary vascularization or heart valve replacement.”
“We are developing a specialized program to treat patients who come in for heart surgery for other conditions like coronary artery disease or heart valve issues and have heart failure,” he said. “We’ll have the technology to care for patients with heart failure at the same time when we’re handling coronary vascularization or heart valve replacement.”
Bypass surgery accounts for approximately 60% of the practices’ work, and Dr. Rokkas also highlighted an innovative technique the team uses for patients who need bypass surgery but who are unable to undergo angioplasty of their coronary arteries.
“These patients require the use of grafts from the legs and arms that is now performed endoscopically without large incisions. The result is faster recovery and less pain for patients,” he said.
Convenient, Quality Clinical and Surgical Care
Dr. Montalto described Dr. Phillip, who has been with Albany Cardiothoracic Surgeons for almost three years, as a provider who has “exceptional surgical skills and has interests in treating ischemic heart disease, valvular heart disease and heart failure.” Dr. Phillip explained the need for the recently established Heart Valve Clinic, which offers a oneday clinic experience for patients who are preparing for a traditional AVR (aortic valve replacement), a TAVR (transcatheter aortic valve replacement), or a mitral valve repair, which is also performed at St. Peter’s Hospital.
“The volume of patients needing an aortic valve replacement is increasing because we’re identifying the disease more frequently and also because we have new therapies to treat it,” Dr. Phillip said. “The TAVR valve is a minimally invasive option that has expanded in use over the last decade. Both AVR and TAVR come with a lot of imaging and preparation to plan for, so it’s much easier for patients and their families to come into the valve clinic and have all that preparation done in a streamlined way in one day,” especially benefitting patients who travel a significant distance to come to St. Peter’s, she added.
Dr. Phillip explained how the convenience of the Heart Valve Clinic also better serves referring providers. “It’s nice for primary care or cardiology providers that are elsewhere to send their patients to us,” she said. “It makes it a lot easier and more familiar for them because the surgeons and cardiologists are centralized here.”
Another way Albany Cardiothoracic Surgeons provides expert yet convenient surgical care for patients is through concomitant procedures, as described by Dr. Helmer, a surgeon with more than 20 years of experience and expertise in heart bypass surgery, heart valve surgery, and other conditions. Some of the heart procedures and surgeries at St. Peter’s can be performed in the same surgery – such as the Maze procedure for ablation of atrial fibrillation – bringing another level of convenience for patients.
provides expert yet convenient surgical care for patients is through concomitant procedures, as described by Dr. Helmer, a surgeon with more than 20 years of experience and expertise in heart bypass surgery, heart valve surgery, and other conditions. Some of the heart procedures and surgeries at St. Peter’s can be performed in the same surgery – such as the Maze procedure for ablation of atrial fibrillation – bringing another level of convenience for patients.
“The Maze procedure can be done in addition to a mitral valve procedure, for example,” said Dr. Helmer. “If somebody has a history of a mitral valve leaking and a history of atrial fibrillation, we can take care of both of those problems at the same time.” Another example would be adding a clip to the left atrial appendage during a Maze procedure, decreasing the chance of a thrombus forming, which can often lead to a stroke. Many patients are also dependent on a pacemaker to help keep their arrhythmia under control, Dr. Helmer explained, and those patients can sometimes experience an infected or faulty lead in the pacemaker, which requires a lead extraction procedure.
“Over time, the lead can get stuck to the blood vessels and removing them has a little bit of a higher risk of trauma to those blood vessels. So, what we do is called a laser lead extraction. There aren’t many people who do this procedure – it’s kind of a rarity,” said Dr. Helmer.
Innovative Treatment Options for Optimized Outcomes
Speaking of her experience at St. Peter’s, Dr. Helmer specifically highlighted the level of care provided by the nursing staff in the operating room, intensive care unit, and the progressive care unit. “The nursing care in those units is phenomenal. They deserve a lot of credit because they do a really good job taking care of our patients,” she said.
Dr. Hasan, a surgeon with over 35 years of experience in complex cardiac surgery, echoed Dr. Helmer’s praise of the team at St. Peter’s. “It could possibly be the nicest place I’ve ever worked,” he shared. “The reason is many-fold, but we have a brilliant group of nurses, physician’s assistants, and nurse practitioners. We have very good coordination with the administration, and with each other.” One way the providers at Albany Cardiothoracic Surgeons excel at providing optimized patient outcomes is by minimizing the risks associated with blood transfusions, which can sometimes lead to immune reactions and other complications such as infections.
Dr. Hasan explained that cardiac surgeons primarily use circulatory support, or a heart lung machine, during heart surgery, which takes over the work of the heart and lungs. The patient’s blood mingles with priming fluid in the machine, which causes hemoglobin levels to drop.
 “The business of keeping that hemoglobin up and avoiding a transfusion involves several people. Once the heart starts to beat again, and we come off the bypass, the blood left in the machine is given back to the patient. It’s a meticulous technique and an expeditious operation,” Dr. Hasan said, adding that patients can also take iron and folic acid supplements as well as medications to stimulate bone marrow ahead of the procedure to help reduce dilution of the blood. These options are beneficial to all patients, he said, but especially those who may have personal or religious reasons to avoid blood transfusions.
“The business of keeping that hemoglobin up and avoiding a transfusion involves several people. Once the heart starts to beat again, and we come off the bypass, the blood left in the machine is given back to the patient. It’s a meticulous technique and an expeditious operation,” Dr. Hasan said, adding that patients can also take iron and folic acid supplements as well as medications to stimulate bone marrow ahead of the procedure to help reduce dilution of the blood. These options are beneficial to all patients, he said, but especially those who may have personal or religious reasons to avoid blood transfusions.
Dr. Hasan also discussed other innovative procedures performed at St. Peter’s that provide better outcomes for patients. The cardiothoracic surgeons offer bypass surgery utilizing the internal mammary artery as opposed to leg veins, which has been shown to prolong survival and reduce re-operations and heart attacks, he said. Additionally, a procedure called valve sparing aortic root replacement allows patients to retain their own valve, rather than use a valve from animal tissue, which deteriorates over time.
Staying at the Cutting Edge of Cardiothoracic Surgery
The need for cardiovascular services in the Capital Region will continue to increase for several reasons, Dr. Montalto emphasized, including both an aging population and patients choosing to wait longer for preventative care compared to pre-pandemic levels. Dr. Montalto said the team at Albany Cardiothoracic Surgeons is preparing to meet this increased need by continuing to focus on minimally invasive techniques as well as the latest technologies.
“Our structural heart cardiac interventionalists are highly trained and experienced in the latest techniques, including TAVR, mitral clip, and Watchmen procedures,” he said. “Our cardiac electrophysiologists are experts at treating abnormal heart rhythms. Additionally, our vascular surgeons are expertly trained and experienced in minimally invasive endovascular surgical repair of aortic aneurysms. Our catheterization labs are stateof- the-art, and our staff is highly trained. We also have an accredited cardiac rehabilitation program to help patients in their recovery.”
For Dr. Montalto, all of this adds up to a skilled team that’s ready to continue providing expert, high-quality and compassionate care patients can depend on. “Our comprehensive cardiovascular program is expanding and fully prepared to meet the needs of patients, both locally and in communities beyond the Capital Region.”
Referrals can be made to Albany Cardiothoracic Surgeons via Epic, or by calling 518-525-2525. The practice is located at 319 S. Manning Blvd., Suite 110A, Albany, NY 12208.
 Center successfully completed Bassett Healthcare Network’s first GORE® EXCLUDER® Thoracoabdominal Branch Endoprosthesis (TAMBE) procedure in October 2025.
Center successfully completed Bassett Healthcare Network’s first GORE® EXCLUDER® Thoracoabdominal Branch Endoprosthesis (TAMBE) procedure in October 2025.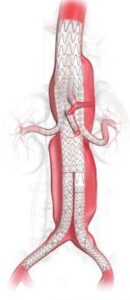 implanted to treat the aneurysm. After the patient is under anesthesia, it is inserted into the body through a small incision and, through the use of needle punctures and imaging, is guided into place.
implanted to treat the aneurysm. After the patient is under anesthesia, it is inserted into the body through a small incision and, through the use of needle punctures and imaging, is guided into place. Private equity (PE) investment in healthcare has grown quickly, reshaping how medical practices run day to day. For physicians and practice owners, selling to a PE firm is a complex decision. It can open doors for growth and support, but it also brings challenges. —offering strategic advantages and potential pitfalls. In New York State, strict regulatory constraints add another layer of complexity that need to be understood before moving forward.
Private equity (PE) investment in healthcare has grown quickly, reshaping how medical practices run day to day. For physicians and practice owners, selling to a PE firm is a complex decision. It can open doors for growth and support, but it also brings challenges. —offering strategic advantages and potential pitfalls. In New York State, strict regulatory constraints add another layer of complexity that need to be understood before moving forward.

