
It didn’t take long for newly named President and CEO Daniel T. Pickett III to begin transforming Albany Med Health System into his vision for the future. Pickett was appointed to the position in December 2025 and recently launched First Choice 2030.
“It’s very simple,” Pickett said of First Choice 2030. “It’s to be the first choice for patient experience, quality and clinical excellence.” The initiative will retain the System’s strengths while honing them to navigate the years ahead. “First Choice 2030 is about Albany Med continuing to be Albany Med and building on its history,” Pickett said. “It’s about positioning Albany Med Health System as the region’s trusted, connected and transformative academic health system.”
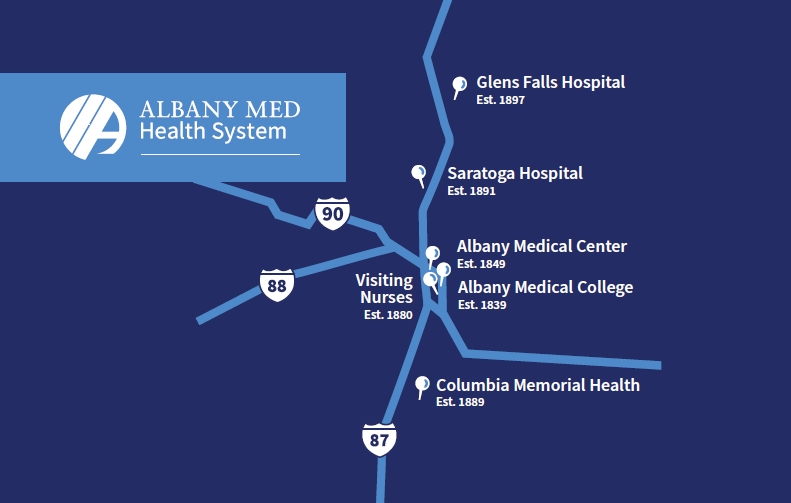
 Albany Med Health System is the largest and only academic health system in northeastern New York and western New England. It includes Albany Medical Center, Albany Medical College, Columbia Memorial Health, Glens Falls Hospital, Saratoga Hospital, and Visiting Nurses.
Albany Med Health System is the largest and only academic health system in northeastern New York and western New England. It includes Albany Medical Center, Albany Medical College, Columbia Memorial Health, Glens Falls Hospital, Saratoga Hospital, and Visiting Nurses.
It comprises 1,520 hospital beds, more than 900 physicians, and the region’s only Level 1 trauma center and children’s hospital. It is the Capital Region’s largest private employer with more than 16,000 employees and more than $6 billion in economic impact.
Pickett has been a part of the Albany Med Health System since 2012, serving on the boards of the Medical Center and Health System, including as the System Board chair.
 “Our first focus is on what’s not going to change,” he said of the First Choice 2030 initiative. “Right now, we have four hospitals, a college, an outpatient practice, visiting nurses. We’ve got almost 1,000 doctors that operate across 100 different points of care. What’s not going to change is our passion for making sure we are operating as effectively as we can. “At the end of the day, if you’re focused on those things and doing them in an efficient way with increasing movement from volume to value, you’ll be a winner, and you’ll be first choice that’s what we’re working toward.”
“Our first focus is on what’s not going to change,” he said of the First Choice 2030 initiative. “Right now, we have four hospitals, a college, an outpatient practice, visiting nurses. We’ve got almost 1,000 doctors that operate across 100 different points of care. What’s not going to change is our passion for making sure we are operating as effectively as we can. “At the end of the day, if you’re focused on those things and doing them in an efficient way with increasing movement from volume to value, you’ll be a winner, and you’ll be first choice that’s what we’re working toward.”
Structured for Success
Albany Med Health System’s structure, including those 100 different points of care, ensures top-notch care. “We have three priorities,” said Pickett. “Patient experience, the quality and the clinical excellence.” Keeping those in mind, the system has been structured so that:
- High-acuity specialty services are centered at Albany Medical Center Hospital.
- Community hospitals, located in Glens Falls, Hudson and Saratoga Springs, provide strong local access and bring clinical specialization.
- Patients can receive high-quality care very close to home, with seamless connection to Albany Medical Center when advanced or complex care is required.
- Subspeciality programs are expanded based on regional demand and community need.
There always will be room for improvement to optimize patient satisfaction and outcomes. As part of introducing himself to staff, Pickett spent hours listening to their feedback about improving the quality of care throughout the Albany Med Health System.
“I’ve been to all of our communities,” he said. “I’ve talked with our team from the executive  level right down to all the different places we support that provide care. My job is to help staff do more of what’s working and unblock the things that aren’t so they can do what they invested an incredible amount of time to do.”
level right down to all the different places we support that provide care. My job is to help staff do more of what’s working and unblock the things that aren’t so they can do what they invested an incredible amount of time to do.”
When all these medical professionals work as a team, first-rate healthcare is the result. For example, Albany Med is the region’s only academic health system. That means the System cares for the most complex and high-risk patients, cases that other hospitals are not equipped to manage.
In addition, the demand for emergency services continues to grow in the Capital Region. As a result, Albany Medical Center Hospital is responding with plans to expand and enhance its adult trauma center. The project marks the first expansion of the hospital’s adult emergency department in 20 years.
“At the time of our last expansion, we saw an average of 57,000 patients per year,” said Denis Pauze, MD, chair of Albany Medical Center’s Department of Emergency Medicine. “Now, we are approaching 85,000. Growing our emergency department allows us to continue meeting that need for our patients, and the other hospitals who rely on us as well.”
Announced in July 2025, the $25 million project aims to add 7,000 square feet, increasing its footprint by nearly 25 percent and direct patient care space by 50 percent.
Albany Medical Center is the busiest trauma center in New York state, and the region’s only Level 1 adult and pediatric trauma center. The expansion project is expected to include:
- More than 20 patient care rooms and an additional care zone for the most critically ill and complex patients, allowing for more seamless and appropriate care.
- A redesigned triage area allowing faster assessment and prioritization of patients based on the severity of their conditions, resulting in enhanced patient safety.
- An increase from two trauma bays to five, increasing capacity, improving efficiency, and enabling teams to concurrently treat multiple trauma patients.
- Plans for dedicated geriatric care space.
 Even before construction is complete, Albany Medical Center has implemented changes to care, including decreased wait times. “Not only are we growing to meet our mission—we continuously strive to improve upon how we deliver our mission,” said Jason Mouzakes, MD, president and CEO of Albany Medical Center Hospital. “Rethinking the blueprint for our emergency department and how patients move from arrival through discharge or hospital admission will allow us to transform the patient
Even before construction is complete, Albany Medical Center has implemented changes to care, including decreased wait times. “Not only are we growing to meet our mission—we continuously strive to improve upon how we deliver our mission,” said Jason Mouzakes, MD, president and CEO of Albany Medical Center Hospital. “Rethinking the blueprint for our emergency department and how patients move from arrival through discharge or hospital admission will allow us to transform the patient
experience.”
Other innovative changes to care delivery include a tiered triage response system deploying hospital-wide nurses and doctors during peak volumes, and a strengthened workforce through strategic recruitment and retention efforts with local nursing schools.
Farther north, Glens Falls Hospital’s Emergency Department will undergo its own expansion to improve patient experience, patient flow, and patient outcomes. Construction is already underway to the Sheridan Emergency Department.
Enhancements include an additional 7,000 square feet, a dedicated CT scanner to help providers diagnose and treat patients faster and nearly double the number of rooms for the most seriously ill and behavioral health patients. Patients with more minor illnesses and injuries will have a dedicated treatment area, helping all patients receive the most efficient care possible.
“The Glens Falls Hospital Emergency Department is a truly invaluable regional resource, but in the three decades since the department was last renovated, the needs and expectations of patients—and the best practices and technologies of emergency medicine—have changed greatly,”said Paul Scimeca, president and CEO of Glens Falls Hospital. “This transformation will create the optimal physical space for our staff’s diagnostic and treatment expertise and skills while also enhancing our patients’ comfort, privacy, and personalized experience.”
Construction on both facilities is expected to be completed by the end of 2026.

Providing Pediatric Care
Albany Medical Center Hospital recognizes the importance of caring for children who are ill, at risk or in need of acute care. Albany Med operates the region’s only children’s hospital, pediatric emergency department, childhood cancer center, pediatric intensive care unit, and Level IV NICU.
 Established in 1986, the Bernard & Millie Duker Children’s Hospital contains 125 beds devoted exclusively to the medical needs of patients under 18 years of age. It is the referral center for all seriously ill and injured children from 25 counties across upstate New York and western New England.
Established in 1986, the Bernard & Millie Duker Children’s Hospital contains 125 beds devoted exclusively to the medical needs of patients under 18 years of age. It is the referral center for all seriously ill and injured children from 25 counties across upstate New York and western New England.
The children’s hospital is staffed by more than 140 physicians trained in 40 subspecialties, and more than 400 pediatric nurses, therapists, social workers, and child-life specialists. “The Bernard & Millie Duker Children’s Hospital, the region’s only children’s hospital, is a place we hope you never have to visit,” said Barbara E. Ostrov, MD, chief of service at the children’s hospital. “We take tremendous pride in knowing we are here in case your child should ever need world-class care, close to home.”
Implementing First Choice 2030 will require a leadership team well-versed in healthcare strategies. In January 2026, Tony James was named executive vice president of strategy, transformation, and corporate development.
“The Albany Med Health System is renowned in the Capital Region and beyond for its quality of care and the clinical expertise of its providers,” James said. “As the system continues to evolve and mature, I’m looking forward to developing and implementing strategies and solutions that will ensure we can continue to offer the highest quality and most efficient care to best serve the people of our communities and everyone who needs our services.”
In March, Jason Mouzakes, MD, was named president of Albany Medical Center Hospital. As such, he will oversee hospital operations, clinical strategy, workforce development, and quality and safety performance. He will be pivotal in advancing First Choice 2030.
“I am inspired every day by the talent, dedication and compassion of our teams,” Mouzakes said. “Together, we will advance First Choice 2030 by delivering exceptional quality, improving the patient and family experience, and ensuring access to the most advanced academic and specialty care for the communities we serve.”
The next step for First Choice 2030 is to align System hospitals around the new shared vision, mission, and strategy. That includes operating as one coordinated enterprise across all hospitals, while standardizing best practices in safety, quality, and patient experience.
For example, plans call for service line integration to improve referral pathways and connect patients with Albany Medical Center for complex and high-acuity care.
“Our goal is clear: To become the region’s trusted, connected and transformative academic health system — where excellence is measurable, access is seamless and alignment drives results,” Pickett said.
 For as long as he can remember, Dr. Martin “Marty” Stallone has held two unwavering truths: he wanted to be a physician, and he wanted to serve his country. Both were anchored by clear purpose.
For as long as he can remember, Dr. Martin “Marty” Stallone has held two unwavering truths: he wanted to be a physician, and he wanted to serve his country. Both were anchored by clear purpose.
 how care is delivered and where it often breaks down. He saw firsthand the pressures facing providers, the operational realities behind clinical decisions, and the importance of aligning strategy with real-world practice.
how care is delivered and where it often breaks down. He saw firsthand the pressures facing providers, the operational realities behind clinical decisions, and the importance of aligning strategy with real-world practice. Latham, NY, and founded more than 40 years ago by local physicians committed to doing what’s right for the community. Already familiar with – and impressed by – the organization’s long-standing focus on keeping patients at the center of care, Dr. Stallone saw an opportunity to help advance that mission even further.
Latham, NY, and founded more than 40 years ago by local physicians committed to doing what’s right for the community. Already familiar with – and impressed by – the organization’s long-standing focus on keeping patients at the center of care, Dr. Stallone saw an opportunity to help advance that mission even further. At the core of his vision is partnership. Drawing on his experience as both a physician and a former health system CEO, Stallone sees collaboration as the most effective path forward in an increasingly complex healthcare environment. He designs practical, sustainable, and impactful programs by grounding his strategy in the real challenges facing the healthcare system, including rising costs.
At the core of his vision is partnership. Drawing on his experience as both a physician and a former health system CEO, Stallone sees collaboration as the most effective path forward in an increasingly complex healthcare environment. He designs practical, sustainable, and impactful programs by grounding his strategy in the real challenges facing the healthcare system, including rising costs. independent multi specialty medical practice. In 2022, CDPHP and Community Care Physicians took a bold step to transform care for thousands of Capital Region residents, creating a more seamless, coordinated experience for both patients and their providers.
independent multi specialty medical practice. In 2022, CDPHP and Community Care Physicians took a bold step to transform care for thousands of Capital Region residents, creating a more seamless, coordinated experience for both patients and their providers.



 “The team’s surgical expertise enables them to not only perform traditional CABG (coronary artery bypass graft) procedures, but also virtually any complex cardiac condition,” explained Dr. Montalto. “Our surgeons specialize in repair and replacement of mitral and aortic valves as well as surgery for aortic aneurysms. This expertise is why St. Peter’s cardiac surgery is consistently ranked among the highest quality programs in New York state.”
“The team’s surgical expertise enables them to not only perform traditional CABG (coronary artery bypass graft) procedures, but also virtually any complex cardiac condition,” explained Dr. Montalto. “Our surgeons specialize in repair and replacement of mitral and aortic valves as well as surgery for aortic aneurysms. This expertise is why St. Peter’s cardiac surgery is consistently ranked among the highest quality programs in New York state.” “We are developing a specialized program to treat patients who come in for heart surgery for other conditions like coronary artery disease or heart valve issues and have heart failure,” he said. “We’ll have the technology to care for patients with heart failure at the same time when we’re handling coronary vascularization or heart valve replacement.”
“We are developing a specialized program to treat patients who come in for heart surgery for other conditions like coronary artery disease or heart valve issues and have heart failure,” he said. “We’ll have the technology to care for patients with heart failure at the same time when we’re handling coronary vascularization or heart valve replacement.” provides expert yet convenient surgical care for patients is through concomitant procedures, as described by Dr. Helmer, a surgeon with more than 20 years of experience and expertise in heart bypass surgery, heart valve surgery, and other conditions. Some of the heart procedures and surgeries at St. Peter’s can be performed in the same surgery – such as the Maze procedure for ablation of atrial fibrillation – bringing another level of convenience for patients.
provides expert yet convenient surgical care for patients is through concomitant procedures, as described by Dr. Helmer, a surgeon with more than 20 years of experience and expertise in heart bypass surgery, heart valve surgery, and other conditions. Some of the heart procedures and surgeries at St. Peter’s can be performed in the same surgery – such as the Maze procedure for ablation of atrial fibrillation – bringing another level of convenience for patients. “The business of keeping that hemoglobin up and avoiding a transfusion involves several people. Once the heart starts to beat again, and we come off the bypass, the blood left in the machine is given back to the patient. It’s a meticulous technique and an expeditious operation,” Dr. Hasan said, adding that patients can also take iron and folic acid supplements as well as medications to stimulate bone marrow ahead of the procedure to help reduce dilution of the blood. These options are beneficial to all patients, he said, but especially those who may have personal or religious reasons to avoid blood transfusions.
“The business of keeping that hemoglobin up and avoiding a transfusion involves several people. Once the heart starts to beat again, and we come off the bypass, the blood left in the machine is given back to the patient. It’s a meticulous technique and an expeditious operation,” Dr. Hasan said, adding that patients can also take iron and folic acid supplements as well as medications to stimulate bone marrow ahead of the procedure to help reduce dilution of the blood. These options are beneficial to all patients, he said, but especially those who may have personal or religious reasons to avoid blood transfusions. Center successfully completed Bassett Healthcare Network’s first GORE® EXCLUDER® Thoracoabdominal Branch Endoprosthesis (TAMBE) procedure in October 2025.
Center successfully completed Bassett Healthcare Network’s first GORE® EXCLUDER® Thoracoabdominal Branch Endoprosthesis (TAMBE) procedure in October 2025.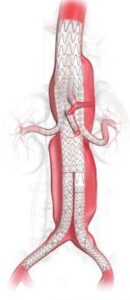 implanted to treat the aneurysm. After the patient is under anesthesia, it is inserted into the body through a small incision and, through the use of needle punctures and imaging, is guided into place.
implanted to treat the aneurysm. After the patient is under anesthesia, it is inserted into the body through a small incision and, through the use of needle punctures and imaging, is guided into place. Private equity (PE) investment in healthcare has grown quickly, reshaping how medical practices run day to day. For physicians and practice owners, selling to a PE firm is a complex decision. It can open doors for growth and support, but it also brings challenges. —offering strategic advantages and potential pitfalls. In New York State, strict regulatory constraints add another layer of complexity that need to be understood before moving forward.
Private equity (PE) investment in healthcare has grown quickly, reshaping how medical practices run day to day. For physicians and practice owners, selling to a PE firm is a complex decision. It can open doors for growth and support, but it also brings challenges. —offering strategic advantages and potential pitfalls. In New York State, strict regulatory constraints add another layer of complexity that need to be understood before moving forward.



 “Our goal is simple: to give patients access to the latest orthopedic innovations as we provide quality and efficient care centered around each patient’s needs,” said Imran Akhtar, DO, who founded the practice with Hamza Murtaza, MD.
“Our goal is simple: to give patients access to the latest orthopedic innovations as we provide quality and efficient care centered around each patient’s needs,” said Imran Akhtar, DO, who founded the practice with Hamza Murtaza, MD.
 Making It Easy for Patients
Making It Easy for Patients Dr. Akhtar, who is board certified, specializes in joint replacement and reconstruction. He completed his residency in orthopedic surgery at the Oklahoma State University – Center for Health Sciences in Tulsa. After finishing his residency, he spent an additional year completing an American Association of Hip and Knee Surgeons Fellowship in Hip and Knee replacement at Desert Orthopedic Center in Las Vegas, Nevada. Dr. Akhtar specializes in minimally invasive hip replacement, which reduces the size of surgical scars and expedites postoperative recovery. He performs direct anterior hip replacements and has an interest in partial knee arthroplasty and robotic assisted knee replacement. “My approach to medicine is rooted in empathy and respect. I treat every patient as I would want my own family to be treated. Listening is at the heart of my practice,” Dr. Akhtar said. “By truly hearing my patients’ concerns, we can build a personalized and effective care plan that supports their recovery and long-term well-being.”
Dr. Akhtar, who is board certified, specializes in joint replacement and reconstruction. He completed his residency in orthopedic surgery at the Oklahoma State University – Center for Health Sciences in Tulsa. After finishing his residency, he spent an additional year completing an American Association of Hip and Knee Surgeons Fellowship in Hip and Knee replacement at Desert Orthopedic Center in Las Vegas, Nevada. Dr. Akhtar specializes in minimally invasive hip replacement, which reduces the size of surgical scars and expedites postoperative recovery. He performs direct anterior hip replacements and has an interest in partial knee arthroplasty and robotic assisted knee replacement. “My approach to medicine is rooted in empathy and respect. I treat every patient as I would want my own family to be treated. Listening is at the heart of my practice,” Dr. Akhtar said. “By truly hearing my patients’ concerns, we can build a personalized and effective care plan that supports their recovery and long-term well-being.”
 Dr. Murtaza brings his expertise in hip and knee surgery to the orthopedic team. He received his medical degree from SUNY Upstate Medical University in Syracuse. He completed a residency in orthopedics at Albany Medical Center, followed by a fellowship in adult reconstruction at NYU Langone Hospital in New York City.
Dr. Murtaza brings his expertise in hip and knee surgery to the orthopedic team. He received his medical degree from SUNY Upstate Medical University in Syracuse. He completed a residency in orthopedics at Albany Medical Center, followed by a fellowship in adult reconstruction at NYU Langone Hospital in New York City. “It is an outstanding organization,” Dr. Angelicola Richardson said, “but, most importantly, the quality of care and the commitment to the community align with my responsibilities to my patients.” Before joining St. Peter’s Orthopedics, Dr. Angelicola-Richardson served patients at Rome Health in Rome, New York, where he was known for his compassionate care and meticulous surgical outcomes.
“It is an outstanding organization,” Dr. Angelicola Richardson said, “but, most importantly, the quality of care and the commitment to the community align with my responsibilities to my patients.” Before joining St. Peter’s Orthopedics, Dr. Angelicola-Richardson served patients at Rome Health in Rome, New York, where he was known for his compassionate care and meticulous surgical outcomes. Dr. Mahjoub’s clinical expertise spans the full spectrum of foot and ankle care. He has specialized training in minimally invasive techniques, ankle arthroscopy, ankle fusion, total ankle replacement, flatfoot reconstruction, and bunion correction. He also treats a wide range of tendon and soft tissue conditions, including disorders of the Achilles and peroneal tendons.
Dr. Mahjoub’s clinical expertise spans the full spectrum of foot and ankle care. He has specialized training in minimally invasive techniques, ankle arthroscopy, ankle fusion, total ankle replacement, flatfoot reconstruction, and bunion correction. He also treats a wide range of tendon and soft tissue conditions, including disorders of the Achilles and peroneal tendons.
 The surgical team uses the latest technologies and techniques to treat patients effectively. That means robotic assisted techniques for joint replacements, minimally invasive procedures, and advanced diagnostics.
The surgical team uses the latest technologies and techniques to treat patients effectively. That means robotic assisted techniques for joint replacements, minimally invasive procedures, and advanced diagnostics. St. Peter’s Orthopedics works with Sunnyview Rehabilitation, which has 12 outpatient clinics throughout Albany, Saratoga, Schenectady, and Renssalaer counties, and is a member of St. Peter’s Health Partners.
St. Peter’s Orthopedics works with Sunnyview Rehabilitation, which has 12 outpatient clinics throughout Albany, Saratoga, Schenectady, and Renssalaer counties, and is a member of St. Peter’s Health Partners. I will not debate the politics behind the recent health care cuts, but I will share my concerns about their impacts.
I will not debate the politics behind the recent health care cuts, but I will share my concerns about their impacts.
